ニボルマブ(オプジーボ)の効果を高める新たな併用療法 [免疫療法]
進行肺癌に対する免疫チェックポイント阻害剤として一番初めに2015年末に登場したニボルマブですが、ペムブロリズマブやアテゾリズマブの登場により、その使用頻度に陰りが見えはじめている印象を受ける今日この頃です(2週毎よりも3週毎の投与間隔の方が医療従事者も患者さんも良いですよね)。 そんな状況を打開すべく、ニボルマブに新たな併用療法の有効性を示す結果が今月号のLancet Oncologyに掲載されました。
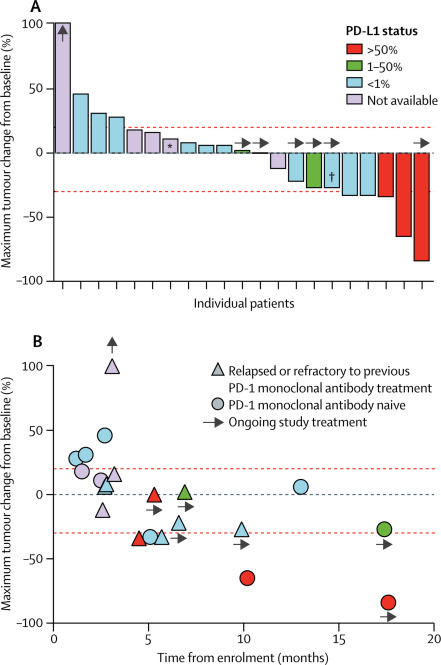
ALT-803(肝機能異常のように見える名前ですね)というIL-15作動薬とニボルマブの併用療法のI相試験の結果ですが、それなりの上乗せ効果があるようです。第Ⅰ相試験なのであくまで参考にしかなりませんが、奏効率は29%、無増悪生存期間中央値は9.4ヶ月なので、意味のある上乗せ効果だと考えますが、実臨床に出てくるのは数年後になりそうです。
ALT-803, an IL-15 superagonist, in combination with nivolumab in patients with metastatic non-small cell lung cancer: a non-randomised, open-label, phase 1b trial
Summary
Background
Immunotherapy with PD-1 or PD-L1 blockade fails to induce a response in about 80% of patients with unselected non-small cell lung cancer (NSCLC), and many of those who do initially respond then develop resistance to treatment. Agonists that target the shared interleukin-2 (IL-2) and IL-15Rβγ pathway have induced complete and durable responses in some cancers, but no studies have been done to assess the safety or efficacy of these agonists in combination with anti-PD-1 immunotherapy. We aimed to define the safety, tolerability, and activity of this drug combination in patients with NSCLC.
Methods
In this non-randomised, open-label, phase 1b trial, we enrolled patients (aged ≥18 years) with previously treated histologically or cytologically confirmed stage IIIB or IV NSCLC from three academic hospitals in the USA. Key eligibility criteria included measurable disease, eligibility to receive anti-PD-1 immunotherapy, and an Eastern Cooperative Oncology Group performance status of 0 or 1. Patients received the anti-PD-1 monoclonal antibody nivolumab intravenously at 3 mg/kg (then 240 mg when US Food and Drug Administration [FDA]-approved dosing changed) every 14 days (either as new treatment or continued treatment at the time of disease progression) and the IL-15 superagonist ALT-803 subcutaneously once per week on weeks 1–5 of four 6-week cycles for 6 months. ALT-803 was administered at one of four escalating dose concentrations: 6, 10, 15, or 20 μg/kg. The primary endpoint was to define safety and tolerability and to establish a recommended phase 2 dose of ALT-803 in combination with nivolumab. Analyses were per-protocol and included any patients who received at least one dose of study treatment. This trial is registered with ClinicalTrials.gov, number NCT02523469; phase 2 enrolment of patients is ongoing.
Findings
Between Jan 18, 2016, and June 28, 2017, 23 patients were enrolled and 21 were treated at four dose levels of ALT-803 in combination with nivolumab. Two patients did not receive treatment because of the development of inter-current illness during enrolment, one patient due to leucopenia and one patient due to pulmonary dysfunction. No dose-limiting toxicities were recorded and the maximum tolerated dose was not reached. The most common adverse events were injection-site reactions (in 19 [90%] of 21 patients) and flu-like symptoms (15 [71%]). The most common grade 3 adverse events, occurring in two patients each, were lymphocytopenia and fatigue. A grade 3 myocardial infarction occurred in one patient. No grade 4 or 5 adverse events were recorded. The recommended phase 2 dose of ALT-803 is 20 μg/kg given once per week subcutaneously in combination with 240 mg intravenous nivolumab every 2 weeks.
Interpretation
ALT-803 in combination with nivolumab can be safely administered in an outpatient setting. The promising clinical activity observed with the addition of ALT-803 to the regimen of patients with PD-1 monoclonal antibody relapsed and refractory disease shows evidence of anti-tumour activity for a new class of agents in NSCLC.
肺がんの治療に疑問を感じたら [肺癌の新治療]

自分が、あるいは家族が肺がんと診断されて治療を受けようとしている方、受けている方がいると思いますが、医療機関から提案された治療に疑問を感じることもあるかもしれません。 日本肺癌学会では、診療ガイドラインを発行しており、毎年情報を更新しています。
https://www.haigan.gr.jp/modules/guideline/index.php?content_id=3
専門外の人でもできるだけ、わかりやすく記載されていますので(作成に関わったスタッフの方々に感謝です)、この情報をもとに自分の病状と合わせて相談をするのが良いと思います。 あくまでもガイドラインですから、このとおりにするのがベストという訳ではありませんので、個々の事情や希望も含め、しっかり納得するまで話し合うことが大事です。
腸内細菌叢が免疫チェックポイント阻害剤の効果に影響する(Scienceより) [免疫療法]
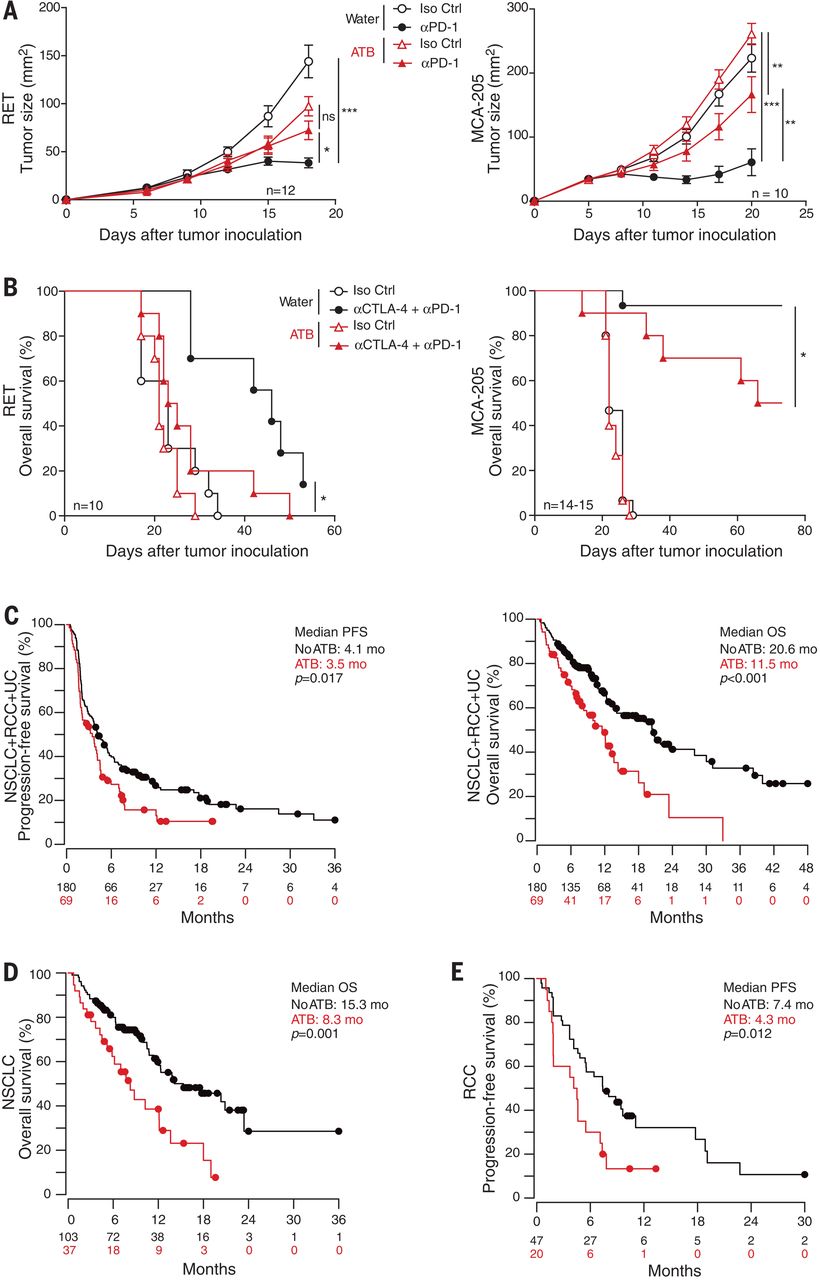
先日、ブログに別の論文をアップしましたが、Scienceでも同様の報告がなされていました。抗生剤を投与し、腸管細菌叢のバランスを崩してしまうと、免疫療法の効果にも影響してしまうという内容です。ただし、抗生剤の投与が必要な患者さんはそうでない患者さんと比較し、全身状態が良くない場合が多いことが推察されるからバイアスがある可能性を念頭に置かねばなりません。しかし、同様の報告がなされている(=再現性がある)ことは、実際に臨床に役立つ情報といえると考えます。 将来的には、健康な方の便をがん患者さんに移植(お尻から注腸するかカプセル化して内服するかでしょうか)する治療法が確立するかもしれませんが、精神的な副作用があるかもしれませんね。いずれにせよ、腸管細菌を良い状態に保つことは健康に良さそうですから、乳製品の摂取など、日々の食生活に気を使うようにしたいものです。
Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors.
Science. 2018 Jan 5;359(6371):91-97. doi: 10.1126/science.aan3706.
Abstract
Immune checkpoint inhibitors (ICIs) targeting the PD-1/PD-L1 axis induce sustained clinical responses in a sizable minority of cancer patients. We found that primary resistance to ICIs can be attributed to abnormal gut microbiome composition. Antibiotics inhibited the clinical benefit of ICIs in patients with advanced cancer. Fecal microbiota transplantation (FMT) from cancer patients who responded to ICIs into germ-free or antibiotic-treated mice ameliorated the antitumor effects of PD-1 blockade, whereas FMT from nonresponding patients failed to do so. Metagenomics of patient stool samples at diagnosis revealed correlations between clinical responses to ICIs and the relative abundance of Akkermansia muciniphila Oral supplementation with A. muciniphila after FMT with nonresponder feces restored the efficacy of PD-1 blockade in an interleukin-12-dependent manner by increasing the recruitment of CCR9+CXCR3+CD4+ T lymphocytes into mouse tumor beds.
肺癌に新たな抗PD-L1抗体、アテゾリズマブ(テセントリク)が登場 [免疫療法]
2018年1月に肺癌患者さんを対象に、ニボルマブ、ペムブロリズマブ(いずれも抗PD-1抗体)に続く、第三の免疫チェックポイント阻害剤であるアテゾリズマブ(テセントリク、抗PD-L1抗体)が日本で承認されました。今月、薬価収載されたことから、いよいよテセントリクが臨床現場でも使われるようになります。
このアテゾリズマブは抗PD-1抗体ではなく「抗PD-L1」抗体です。抗PD-1抗体はTリンパ球表面にあるPD-1タンパクを標的とした抗体薬でしたが、今回の抗PD-L1は腫瘍細胞の表面にあるリガンド(L)タンパクであるPD-L1を標的とした抗体薬です。PD-1とPD-L1が互いに結合することで、腫瘍免疫が機能しなくなってしまう不都合が生じているところを抗PD-1抗体または抗PD-L1抗体を使用し、ブロックすることで、本来患者さん自信に備わっている腫瘍免疫を再活性化する役割を果たす薬剤です。
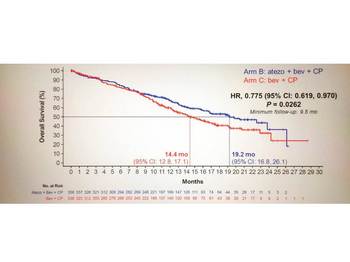
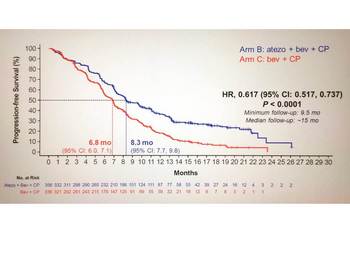
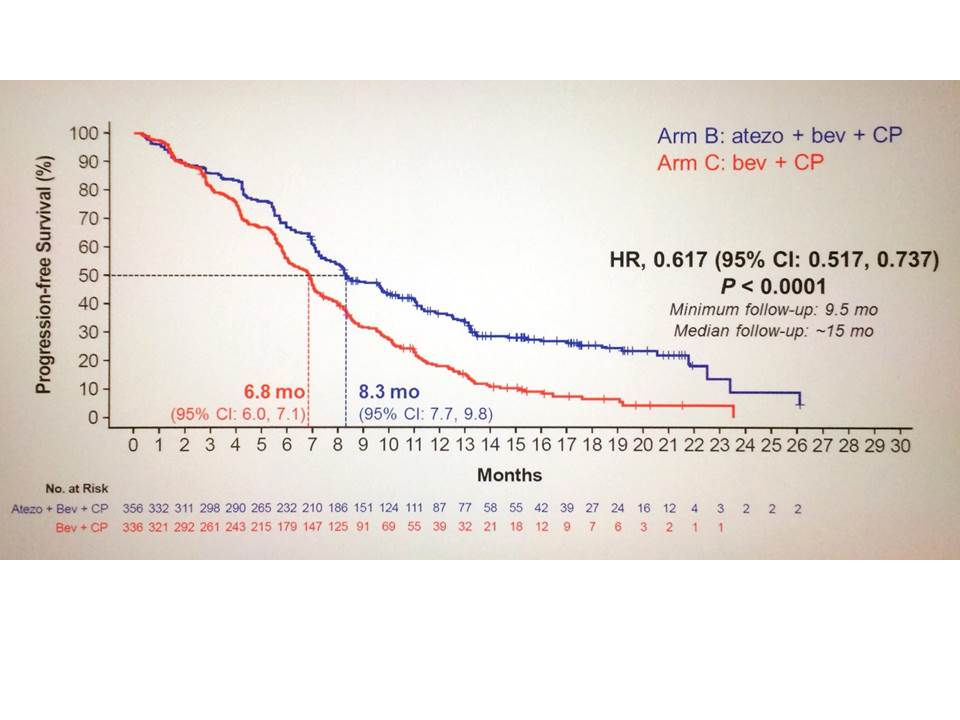
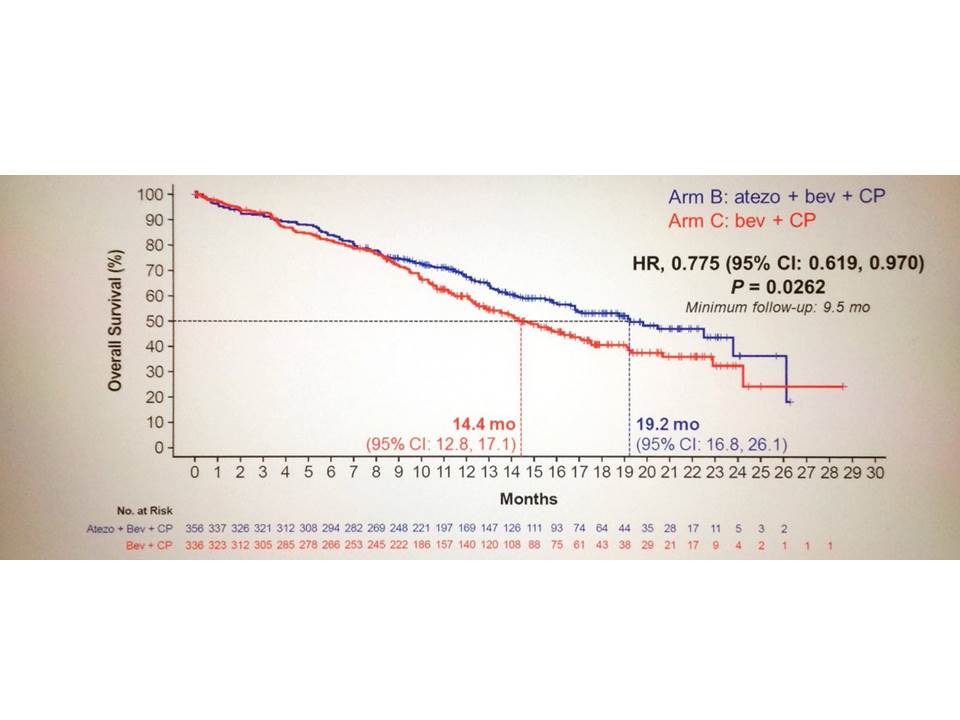
この新薬も承認の根拠となった試験から、まずはプラチナ併用療法後に増悪した二次治療以降で、アテゾリズマブ単剤で使用されることが予想されます。しかし、既に更なる治療戦略は練られており、昨年末には初回治療として化学療法との併用療法で有効性が示されています(IMpower150試験)。2つの図にある生存曲線が、アテゾリズマブと化学療法の併用療法の有効性を示しています。この試験の詳細なデータは夏前までには発表されると思いますが、将来的には早い段階で免疫チェックポイント阻害剤を化学療法などと併用して投与する戦略が推奨されるようになることが予想されるでしょう。
IMpower150試験は、進行または転移性非扁平上皮NSCLC患者1202名を対象に、A群(アテゾリズマブ[1,200mg静注]+カルボプラチン[AUC 6]+パクリタキセル[200mg/m2静注])、B群(アテゾリズマブ[1,200mg静注]+カルボプラチン[AUC 6]+パクリタキセル[200mg/m2静注]+ベバシズマブ[15mg/kg静注])、C群(カルボプラチン[AUC 6]+パクリタキセル[200mg/m2静注]+ベバシズマブ[15mg/kg静注])の3群に1:1:1の割合でランダム化し、各群の投与レジメンに従い3週ごとに治療が実施された。
主要評価項目はEGFR遺伝子変異陽性およびALK融合遺伝子転座陽性を除くITT(Intento to treat)解析集団ならびにT細胞活性調整因子(Teff)の遺伝子発現により層別化した集団におけるPFSおよびITT解析集団における全生存期間(OS)であった。
主要評価項目のEGFR遺伝子変異陽性およびALK融合遺伝子転座陽性を除くITT(Intento to treat)解析集団におけるPFS中央値はアテゾリズマブ併用療法群で8.3ヶ月、対照群で6.8ヶ月と有意にアテゾリズマブ群でPFSの延長を認めた(HR=0.62、95%信頼区間0.52-0.74、p<0.0001)。OS中央値はアテゾリズマブ併用療法群で19.2ヶ月、対照群で14.4ヶ月と有意にアテゾリズマブ群でOSの延長を認めた(HR=0.775、95%信頼区間0.619-0.970、p=0.0262)。
このアテゾリズマブは抗PD-1抗体ではなく「抗PD-L1」抗体です。抗PD-1抗体はTリンパ球表面にあるPD-1タンパクを標的とした抗体薬でしたが、今回の抗PD-L1は腫瘍細胞の表面にあるリガンド(L)タンパクであるPD-L1を標的とした抗体薬です。PD-1とPD-L1が互いに結合することで、腫瘍免疫が機能しなくなってしまう不都合が生じているところを抗PD-1抗体または抗PD-L1抗体を使用し、ブロックすることで、本来患者さん自信に備わっている腫瘍免疫を再活性化する役割を果たす薬剤です。
この新薬も承認の根拠となった試験から、まずはプラチナ併用療法後に増悪した二次治療以降で、アテゾリズマブ単剤で使用されることが予想されます。しかし、既に更なる治療戦略は練られており、昨年末には初回治療として化学療法との併用療法で有効性が示されています(IMpower150試験)。2つの図にある生存曲線が、アテゾリズマブと化学療法の併用療法の有効性を示しています。この試験の詳細なデータは夏前までには発表されると思いますが、将来的には早い段階で免疫チェックポイント阻害剤を化学療法などと併用して投与する戦略が推奨されるようになることが予想されるでしょう。
IMpower150試験は、進行または転移性非扁平上皮NSCLC患者1202名を対象に、A群(アテゾリズマブ[1,200mg静注]+カルボプラチン[AUC 6]+パクリタキセル[200mg/m2静注])、B群(アテゾリズマブ[1,200mg静注]+カルボプラチン[AUC 6]+パクリタキセル[200mg/m2静注]+ベバシズマブ[15mg/kg静注])、C群(カルボプラチン[AUC 6]+パクリタキセル[200mg/m2静注]+ベバシズマブ[15mg/kg静注])の3群に1:1:1の割合でランダム化し、各群の投与レジメンに従い3週ごとに治療が実施された。
主要評価項目はEGFR遺伝子変異陽性およびALK融合遺伝子転座陽性を除くITT(Intento to treat)解析集団ならびにT細胞活性調整因子(Teff)の遺伝子発現により層別化した集団におけるPFSおよびITT解析集団における全生存期間(OS)であった。
主要評価項目のEGFR遺伝子変異陽性およびALK融合遺伝子転座陽性を除くITT(Intento to treat)解析集団におけるPFS中央値はアテゾリズマブ併用療法群で8.3ヶ月、対照群で6.8ヶ月と有意にアテゾリズマブ群でPFSの延長を認めた(HR=0.62、95%信頼区間0.52-0.74、p<0.0001)。OS中央値はアテゾリズマブ併用療法群で19.2ヶ月、対照群で14.4ヶ月と有意にアテゾリズマブ群でOSの延長を認めた(HR=0.775、95%信頼区間0.619-0.970、p=0.0262)。
敗血症性ショック患者に対するステロイドの有効性(NEJMより) [ステロイド]
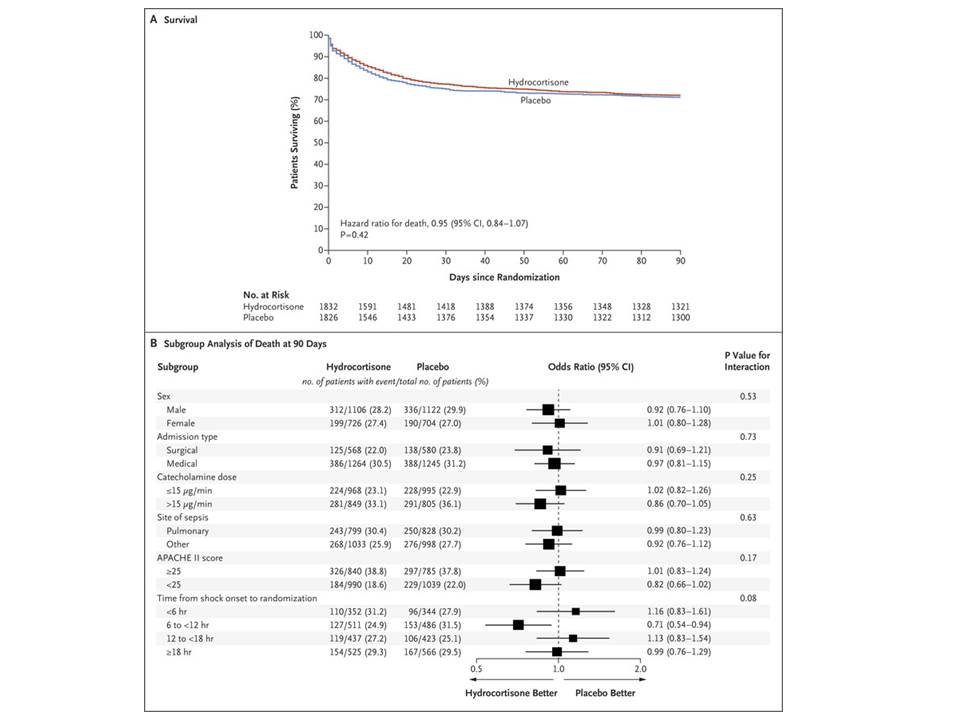
これも2018年3月のNEJMからの報告ですが、臨床現場では敗血症性ショックに陥った患者さんに対するステロイドの有効性に関して議論がありますが、少量投与に肯定的な論調が多いように思います。 Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002 Aug 21;288(7):862-71. Hydrocortisone therapy for patients with septic shock. N Engl J Med. 2008 Jan 10;358(2):111-24. doi: 10.1056/NEJMoa071366. しかし、この論文ではヒドロコルチゾン(コートリル 200 mg/日)の投与が部分的には有益であるが、90 日の時点での全死因死亡は延長しなかったと報告しています。NEJMでは過去の報告も有益ではなかったと報告されています。
背景
ヒドロコルチゾンによって敗血症性ショック患者の死亡率が低下するかどうかは明らかにされていない.
方法
人工呼吸管理を行う予定の敗血症性ショック患者を,ヒドロコルチゾン(200 mg/日)群とプラセボ群に無作為に割り付け,7 日間,または死亡するか集中治療室(ICU)を退室するまで投与した.90 日の時点での全死因死亡を主要評価項目とした.
結果
2013 年 3 月~2017 年 4 月の期間に,3,800 例を無作為化した.主要評価項目の状態が確認されたのは 3,658 例(ヒドロコルチゾン群 1,832 例,プラセボ群 1,826 例)であった.90 日の時点で,ヒドロコルチゾン群の 511 例(27.9%)とプラセボ群の 526 例(28.8%)が死亡していた(オッズ比 0.95,95%信頼区間 [CI] 0.82~1.10,P=0.50).事前に規定した 6 つのサブグループでも,試験レジメンの効果は同様であった.ヒドロコルチゾン群の患者では,プラセボ群の患者よりもショックの消失が早かった(期間の中央値 3 日 [四分位範囲 2~5] 対 4 日 [四分位範囲 2~9],ハザード比 1.32,95% CI 1.23~1.41,P<0.001).ヒドロコルチゾン群の患者では,プラセボ群の患者よりも初回の人工呼吸器装着期間が短かったが(中央値 6 日 [四分位範囲 3~18] 対 7 日 [四分位範囲 3~24],ハザード比 1.13,95% CI 1.05~1.22,P<0.001),再装着を考慮すると,生存し人工呼吸器を装着していない日数に有意差は認められなかった.輸血を受けた患者は,ヒドロコルチゾン群のほうがプラセボ群よりも少なかった(37.0% 対 41.7%,オッズ比 0.82,95% CI 0.72~0.94,P=0.004).28 日死亡率,ショックの再発率,生存し ICU を退室していた日数,生存し退院していた日数,人工呼吸器再装着,腎代替療法の施行率,菌血症または真菌血症の新規発症率に関して,群間で有意差は認められなかった.
結論
人工呼吸管理を行う予定の敗血症性ショック患者において,ヒドロコルチゾンの持続静注により,90 日死亡率がプラセボよりも低くなることはなかった.
未治療EGFR陽性肺がんに対するオシメルチニブ(タグリッソ)の有効性 [EGFR遺伝子変異陽性肺癌]
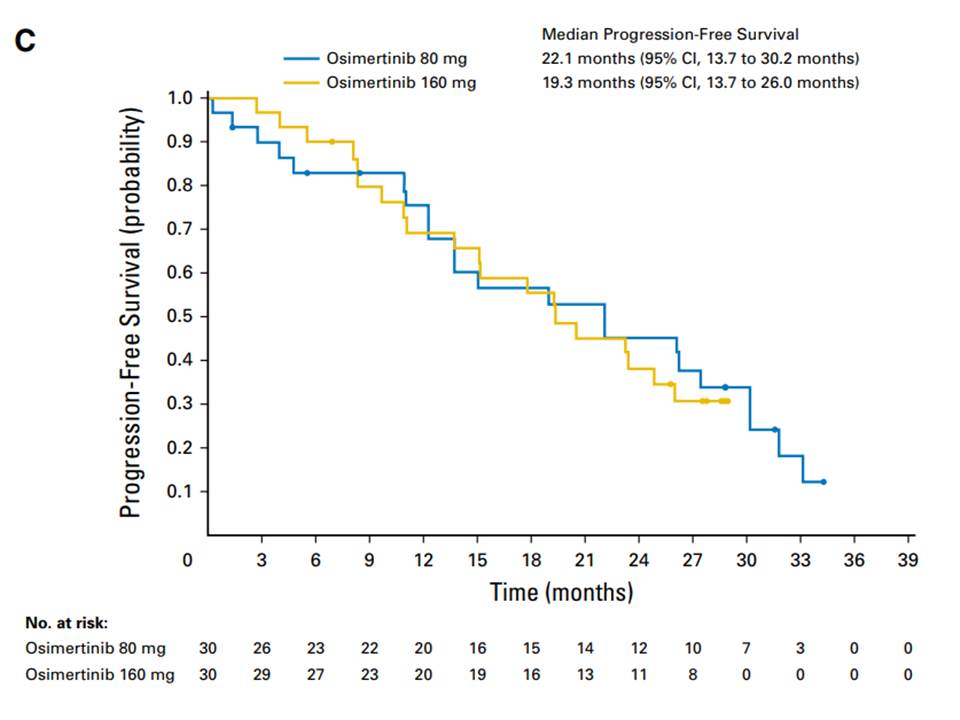
2018年3月号のJCOに未治療EGFR遺伝子変異陽性肺がん患者に対する初回治療としてのオシメルチニブの有効性データが掲載されました。無増悪生存期間中央値は22.1ヶ月で2年に迫る結果です。 日本人では初回治療として第二世代のEGFR-TKIであるアファチニブ(ジオトリフ)を投与した場合、無増悪生存期間中央値は13-16ヶ月であることからさらに半年以上の有効性が期待できる結果となっています。 ただ、現状では、第一世代(ゲフィチニブ、エルロチニブ)または第二世代(アファチニブ)増悪後にT790M耐性変異が認められた場合(約50%の患者さんでみつかります)には二次治療としてオシメルチニブが投与されています。 そこで、 ①初回からオシメルチニブ ②ゲフィチニブ、エルロチニブ、アファチニブのいずれかを使用後、T790M変異を確認してオシメルチニブ のどちらの治療戦略が患者さんにとって有益かとの議論になります。 データを見る限りでは、効果と安全性のバランスから、初回からオシメルチニブを使う方が将来的に増えることが予想されます。
Osimertinib As First-Line Treatment of EGFR Mutation–Positive Advanced Non–Small-Cell Lung Cancer
J Clin Oncol. 2018 Mar 20;36(9):841-849. doi: 10.1200/JCO.2017.74.7576
Abstract
Purpose The AURA study ( ClinicalTrials.gov identifier: NCT01802632) included two cohorts of treatment-naïve patients to examine clinical activity and safety of osimertinib (an epidermal growth factor receptor [EGFR] -tyrosine kinase inhibitor selective for EGFR-tyrosine kinase inhibitor sensitizing [ EGFRm] and EGFR T790M resistance mutations) as first-line treatment of EGFR-mutated advanced non-small-cell lung cancer (NSCLC).
Patients and Methods
Sixty treatment-naïve patients with locally advanced or metastatic EGFRm NSCLC received osimertinib 80 or 160 mg once daily (30 patients per cohort). End points included investigator-assessed objective response rate (ORR), progression-free survival (PFS), and safety evaluation. Plasma samples were collected at or after patients experienced disease progression, as defined by Response Evaluation Criteria in Solid Tumors (RECIST), to investigate osimertinib resistance mechanisms.
Results
At data cutoff (November 1, 2016), median follow-up was 19.1 months. Overall ORR was 67% (95% CI, 47% to 83%) in the 80-mg group, 87% (95% CI, 69% to 96%) in the 160-mg group, and 77% (95% CI, 64% to 87%) across doses. Median PFS time was 22.1 months (95% CI, 13.7 to 30.2 months) in the 80-mg group, 19.3 months (95% CI, 13.7 to 26.0 months) in the 160-mg group, and 20.5 months (95% CI, 15.0 to 26.1 months) across doses. Of 38 patients with postprogression plasma samples, 50% had no detectable circulating tumor DNA. Nine of 19 patients had putative resistance mechanisms, including amplification of MET (n = 1); amplification of EGFR and KRAS (n = 1); MEK1, KRAS, or PIK3CA mutation (n = 1 each); EGFR C797S mutation (n = 2); JAK2 mutation (n = 1); and HER2 exon 20 insertion (n = 1). Acquired EGFR T790M was not detected.
Conclusion
Osimertinib demonstrated a robust ORR and prolonged PFS in treatment-naïve patients with EGFRm advanced NSCLC. There was no evidence of acquired EGFR T790M mutation in postprogression plasma samples.
抗生物質が免疫療法の効果に影響を与える [免疫療法]
Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small cell lung cancer.
Ann Oncol. 2018 Mar 30. doi: 10.1093/annonc/mdy103.
最近、免疫療法の分野では腸管内の細菌叢(マイクロバイオーム)と免疫療法の有効性の効果が関連していることが注目されています。 抗生物質は一般的に、腸内細菌のバランスを崩すことが知られており(なので、抗生剤で下痢をする方もいますよね)、今回の論文は免疫療法の効果を減弱させてしまう可能性を示唆しています。
Abstract
BACKGROUND:
The composition of gut microbiota affects anti-tumor immune responses, preclinical and clinical outcome following immune checkpoint inhibitors (ICI) in cancer. Antibiotics (ATB) alter gut microbiota diversity and composition leading to dysbiosis, which may affect effectiveness of ICI.
PATIENTS AND METHODS:
We examined patients with advanced renal cell carcinoma (RCC) and non-small cell lung cancer (NSCLC) treated with anti-PD-(L)1 mAb monotherapy or combination at two academic institutions. Those receiving ATB within 30 days of beginning ICI were compared to those who did not. Objective response, progression-free survival (PFS) determined by RECIST1.1 and overall survival (OS) were assessed.
RESULTS:
Sixteen of 121 (13%) RCC patients and 48 of 239 (20%) NSCLC patients received ATB. The most common ATB were β-lactam or quinolones for pneumonia or urinary tract infections. In RCC patients, ATB compared to no ATB was associated with increased risk of primary progressive disease (PD) (75% vs 22%, p < 0.01), shorter PFS (median 1.9 vs 7.4 months, hazard ratio (HR) 3.1, 95% confidence interval (CI) 1.4-6.9, p < 0.01), and shorter OS (median 17.3 vs 30.6 months, HR 3.5, 95% CI 1.1-10.8, p = 0.03). In NSCLC patients, ATB was associated with similar rates of primary PD (52% vs 43%, p = 0.26) but decreased PFS (median 1.9 vs 3.8 months, HR 1.5, 95% CI 1.0-2.2, p = 0.03) and OS (median 7.9 vs 24.6 months, HR 4.4, 95% CI 2.6-7.7, p < 0.01). In multivariate analyses, the impact of ATB remained significant for PFS in RCC and for OS in NSCLC.
CONCLUSION:
ATB were associated with reduced clinical benefit from ICI in RCC and NSCLC. Modulatation of ATB-related dysbiosis and gut microbiota composition may be a strategy to improve clinical outcomes with ICI.
Ann Oncol. 2018 Mar 30. doi: 10.1093/annonc/mdy103.
最近、免疫療法の分野では腸管内の細菌叢(マイクロバイオーム)と免疫療法の有効性の効果が関連していることが注目されています。 抗生物質は一般的に、腸内細菌のバランスを崩すことが知られており(なので、抗生剤で下痢をする方もいますよね)、今回の論文は免疫療法の効果を減弱させてしまう可能性を示唆しています。
Abstract
BACKGROUND:
The composition of gut microbiota affects anti-tumor immune responses, preclinical and clinical outcome following immune checkpoint inhibitors (ICI) in cancer. Antibiotics (ATB) alter gut microbiota diversity and composition leading to dysbiosis, which may affect effectiveness of ICI.
PATIENTS AND METHODS:
We examined patients with advanced renal cell carcinoma (RCC) and non-small cell lung cancer (NSCLC) treated with anti-PD-(L)1 mAb monotherapy or combination at two academic institutions. Those receiving ATB within 30 days of beginning ICI were compared to those who did not. Objective response, progression-free survival (PFS) determined by RECIST1.1 and overall survival (OS) were assessed.
RESULTS:
Sixteen of 121 (13%) RCC patients and 48 of 239 (20%) NSCLC patients received ATB. The most common ATB were β-lactam or quinolones for pneumonia or urinary tract infections. In RCC patients, ATB compared to no ATB was associated with increased risk of primary progressive disease (PD) (75% vs 22%, p < 0.01), shorter PFS (median 1.9 vs 7.4 months, hazard ratio (HR) 3.1, 95% confidence interval (CI) 1.4-6.9, p < 0.01), and shorter OS (median 17.3 vs 30.6 months, HR 3.5, 95% CI 1.1-10.8, p = 0.03). In NSCLC patients, ATB was associated with similar rates of primary PD (52% vs 43%, p = 0.26) but decreased PFS (median 1.9 vs 3.8 months, HR 1.5, 95% CI 1.0-2.2, p = 0.03) and OS (median 7.9 vs 24.6 months, HR 4.4, 95% CI 2.6-7.7, p < 0.01). In multivariate analyses, the impact of ATB remained significant for PFS in RCC and for OS in NSCLC.
CONCLUSION:
ATB were associated with reduced clinical benefit from ICI in RCC and NSCLC. Modulatation of ATB-related dysbiosis and gut microbiota composition may be a strategy to improve clinical outcomes with ICI.
MET Exon 14 skipping とMET阻害薬 [肺癌の新治療]
肺腺癌の4%程度の患者さんにMET Exon14 skipping mutationという変異があることが最近報告
されており、この変異を有する患者さんはMET阻害薬が奏効することが示唆されています。
肺癌を扱う国際学術誌の一つであるJCOにその変異を有する患者の特徴が報告されました。
MET Exon 14 Mutations in Non–Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression
・6376例の癌検体を次世代シーケンサーで解析
・上記解析結果をEGFR遺伝子変異陽性肺癌、KRAS遺伝子変異陽性肺癌と比較した
・3%(28/933)の非扁平上皮非小細胞肺癌(NonSq-NSCLC)でMET exon 14 skipping 変異を認めた
・変異陽性患者は高齢者が多い(中央値72.5歳)
・68%が女性、36%が非喫煙者
・早期癌より進行癌の方がMET増幅を有し、cMETのIHCが強陽性となる症例が多い
・これらの多くがcMET阻害薬であるクリゾチニブが奏効していた
MET Exon 14 変異を有する患者にはクリゾチニブ(ザーコリ)が有用である可能性が示唆されます。
マクロCK血症 [肺癌に関わるトピックス]
肺癌などの悪性腫瘍や膠原病を有する患者さんでは筋肉のマーカー(酵素)の一つであるCK(クレアチニンキナーゼ)が高値の患者さんがいます。その場合、どこの筋肉由来かを評価するためにCK分画を測定することがあります。CKのアイソザイムとしてはCK-BB, CK-MB, CK-MMの3つが存在し、BBは急性脳損傷、中枢神経術後、悪性腫瘍で、MBは心筋梗塞などの心疾患、MMは横紋筋融解症や挫滅症候群、筋炎などで上昇します。
しかし、これら3種類のアイソザイムの他に電気泳動上、異なるバンドがみられることがあり、それをマクロCKと呼び、マクロCKは悪性腫瘍や膠原病でみられることがあります。
マクロCKはCK分子が巨大分子化したもので、①免疫グロブリンとの結合、②免疫グロブリン以外のリポ蛋白や多糖体などとの結合が原因と言われています。
しかし、これら3種類のアイソザイムの他に電気泳動上、異なるバンドがみられることがあり、それをマクロCKと呼び、マクロCKは悪性腫瘍や膠原病でみられることがあります。
マクロCKはCK分子が巨大分子化したもので、①免疫グロブリンとの結合、②免疫グロブリン以外のリポ蛋白や多糖体などとの結合が原因と言われています。
治験に参加したい方へ [治験]
現在実施中の治験がわかるサイトをご紹介します。
各種がんで新しい治療にチャレンジをしたい方はご参照ください。
治験に参加することで、負担軽減費(治療費や交通費を負担する)が支払われることが多いので、経済的なメリットもあります。
オンコロ
https://oncolo.jp/
各種がんで新しい治療にチャレンジをしたい方はご参照ください。
治験に参加することで、負担軽減費(治療費や交通費を負担する)が支払われることが多いので、経済的なメリットもあります。
オンコロ
https://oncolo.jp/



